
Thyroid Disorders and Fertility: How Hypothyroidism and Hashimoto’s Can Affect Conception
How Hypothyroidism and Hashimoto’s Can Affect Ovulation, Conception, and Pregnancy

Difficulty getting pregnant is not always caused by abnormalities within the reproductive organs themselves. Fertility depends on coordinated communication between the brain, thyroid, immune system, metabolism, ovaries, and reproductive hormones. When these systems become dysregulated, ovulation, implantation, and early pregnancy signaling may be affected long before overt disease develops.
Thyroid disorders are among the most common endocrine conditions associated with infertility, ovulatory dysfunction, recurrent miscarriage, and implantation difficulties. Both hypothyroidism and autoimmune thyroid conditions such as Hashimoto’s thyroiditis can interfere with reproductive physiology by altering hormone signaling, metabolic regulation, immune balance, and cellular energy production (1).
Importantly, thyroid-related fertility issues are not always identified through routine screening alone. Many women experiencing infertility, irregular ovulation, recurrent pregnancy loss, or persistent difficulty getting pregnant are told their thyroid labs are “normal,” despite persistent symptoms and ongoing reproductive dysfunction. This is because fertility depends not only on circulating thyroid hormone levels, but also on how effectively thyroid hormones are converted, transported, and utilized within reproductive tissues (2).
Even subtle reductions in thyroid hormone activity may influence:
Ovulation timing
Follicle development
Progesterone production
Endometrial receptivity
Implantation
Early pregnancy support
These effects may occur even when menstrual cycles appear regular and standard thyroid laboratory values remain within reference ranges (3).
How Can Thyroid Disorders Affect Fertility?
Thyroid disorders can impair fertility by disrupting ovulation, menstrual cycle regulation, implantation, progesterone production, and early pregnancy signaling. Hypothyroidism and Hashimoto’s thyroiditis have been associated with infertility, miscarriage risk, luteal phase dysfunction, irregular ovulation, and impaired reproductive hormone signaling—even when thyroid laboratory values appear within conventional reference ranges (4).
This article examines how thyroid dysfunction, thyroid autoimmunity, inflammation, and tissue-level hormone signaling may influence fertility outcomes, reproductive hormone regulation, implantation, and pregnancy physiology through a systems-based lens.
How Thyroid Hormones Affect Ovulation, Implantation, and Fertility
Fertility depends on coordinated communication between the brain, thyroid gland, ovaries, adrenal system, immune system, and reproductive hormones. Thyroid hormones play a central role in this process by regulating metabolic activity, cellular energy production, hormone signaling, and tissue responsiveness throughout the reproductive system (1).
Although thyroid hormones are not considered primary reproductive hormones themselves, they strongly influence whether reproductive physiology can proceed efficiently under current metabolic and physiologic conditions. Ovulation, implantation, endometrial development, progesterone production, and early pregnancy support all require adequate thyroid hormone activity at the tissue level (5).
When thyroid signaling becomes impaired, the body may shift away from reproduction as a physiologic priority. This can occur not only in overt hypothyroidism, but also in more subtle states involving impaired thyroid hormone conversion, autoimmune thyroid activity, inflammation, metabolic stress, or reduced tissue responsiveness to thyroid hormones.
In many women, these changes develop gradually and may contribute to:
Irregular ovulation
Delayed ovulation
Luteal phase dysfunction
Reduced implantation support
Difficulty getting pregnant
Increased risk of early pregnancy loss
These patterns may emerge even when menstrual cycles appear relatively regular and standard thyroid laboratory values remain within conventional reference ranges (6).
→ Women’s Hormone & Reproductive Health
Thyroid Hormones as Metabolic Regulators of Reproduction
Reproduction is metabolically demanding. Follicle development, ovulation, implantation, placental development, and early pregnancy all require substantial cellular energy production, oxygen utilization, mitochondrial activity, and nutrient availability. Thyroid hormones help regulate these processes by controlling how efficiently cells generate and utilize energy (5).
When thyroid hormone activity declines, the body may interpret the physiologic environment as unfavorable for reproduction. From a survival perspective, reproduction becomes less biologically prioritized during periods of metabolic stress or reduced energy availability.
As thyroid signaling becomes impaired, this may contribute to:
Suppression of ovulatory signaling
Altered timing of LH and FSH release
Reduced ovarian responsiveness
Impaired endometrial preparation
Decreased progesterone production after ovulation
These changes are often functional and regulatory rather than structural, which helps explain why thyroid-related infertility may develop gradually and remain difficult to identify during routine fertility evaluation (7).
Why Even Mild Thyroid Dysfunction Can Affect Fertility
The reproductive system is highly sensitive to relatively small changes in thyroid hormone activity. Even mild thyroid dysfunction or subclinical hypothyroidism may interfere with reproductive hormone signaling, ovulation timing, implantation physiology, and menstrual cycle regulation (3).
This helps explain why some women experience infertility, recurrent miscarriage, or persistent difficulty getting pregnant despite thyroid laboratory values that fall within standard reference ranges. Reproductive tissues depend not only on circulating thyroid hormone levels, but also on local hormone conversion, receptor sensitivity, cellular uptake, and tissue responsiveness (8).
As a result, thyroid-related reproductive dysfunction is often functional rather than absolute. Ovulation may still occur, menstrual cycles may still appear “normal,” and standard screening may not identify obvious thyroid disease—while tissue-level reproductive signaling remains impaired.
How Hypothyroidism Can Disrupt Ovulation and Menstrual Cycle Regulation
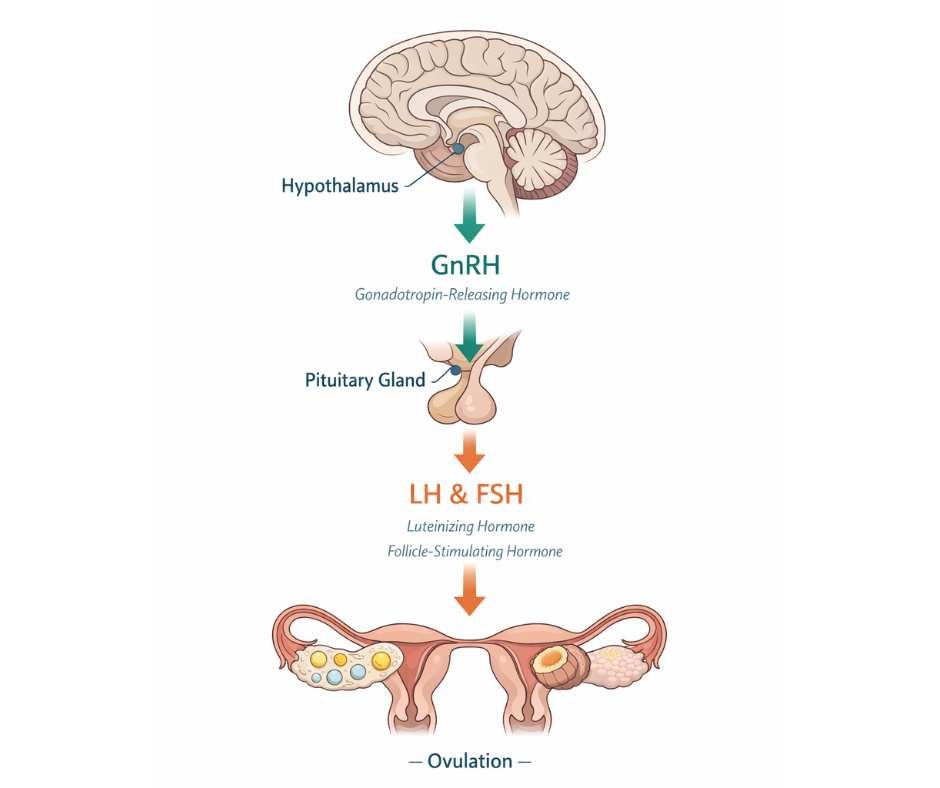
Ovulation depends on coordinated communication between the brain, pituitary gland, ovaries, thyroid hormones, and reproductive signaling pathways. This communication occurs through the hypothalamic–pituitary–ovarian (HPO) axis, which regulates follicle development, ovulation timing, progesterone production, and menstrual cycle function (9).
At the center of this system, the hypothalamus releases gonadotropin-releasing hormone (GnRH), which acts as a regulatory signal to the pituitary gland. In response, the pituitary releases luteinizing hormone (LH) and follicle-stimulating hormone (FSH), the hormones responsible for stimulating follicle maturation and triggering ovulation.
Thyroid hormones help regulate this process indirectly by influencing metabolic activity, mitochondrial energy production, nervous system signaling, and tissue responsiveness to reproductive hormones. When thyroid hormone activity becomes impaired, the timing, intensity, and coordination of ovulatory signaling may become less stable—even when reproductive hormone levels appear within standard laboratory reference ranges (10).
How Hypothyroidism Can Affect Brain–Ovary Communication
In hypothyroidism, reduced thyroid hormone activity may interfere with normal HPO axis signaling in several ways, including:
Altered pulsatile release of GnRH from the hypothalamus
Reduced pituitary responsiveness to hormonal signaling
Disrupted LH and FSH coordination required for ovulation
Impaired follicle maturation within the ovaries
Reduced ovarian responsiveness to reproductive hormones
As these signaling patterns become less coordinated, ovulation may become delayed, irregular, inconsistent, or absent altogether (11).
In some women, this may contribute to:
Irregular menstrual cycles
Longer menstrual cycles
Missed ovulation
Reduced fertility
Difficulty getting pregnant
Subfertility despite apparently “normal” cycles
Functional Ovulatory Dysfunction in Hypothyroidism
Hypothyroidism does not always cause complete anovulation. In many women, ovulation still occurs, but reproductive signaling becomes functionally suboptimal.
This may include:
Delayed ovulation that shortens the fertile window
Weakened luteal phase support after ovulation
Reduced progesterone production
Impaired endometrial preparation for implantation
Less stable hormonal signaling during early pregnancy
These changes may reduce the likelihood of conception and increase the risk of implantation difficulties or early pregnancy loss, even when menstrual cycles appear outwardly regular (5).
Why Thyroid-Related Ovulatory Dysfunction Is Often Missed
Standard fertility evaluations often focus primarily on whether ovulation occurs at all rather than whether ovulation occurs consistently, predictably, and with adequate hormonal support.
Because hypothyroidism-related ovulatory dysfunction is frequently functional rather than absolute, many women may continue menstruating regularly while still experiencing impaired reproductive signaling, reduced implantation support, or difficulty conceiving (6).
This helps explain why thyroid-related infertility is often overlooked during routine fertility screening—particularly in women with subclinical hypothyroidism, Hashimoto’s thyroiditis, or “normal” thyroid laboratory values that do not fully reflect tissue-level thyroid hormone activity.
Hashimoto’s Thyroiditis, Thyroid Antibodies, and Fertility
Thyroid-related infertility is not caused by thyroid hormone levels alone. In many women, autoimmune thyroid activity plays an independent role in ovulation, implantation, early pregnancy support, and reproductive outcomes.
Hashimoto’s thyroiditis—the most common autoimmune thyroid condition—is characterized by immune activity directed against thyroid tissue, often involving thyroid peroxidase (TPO) antibodies and thyroglobulin antibodies. These antibodies reflect ongoing immune dysregulation and inflammatory signaling rather than simply indicating the presence or absence of thyroid disease (12).
Importantly, many women with Hashimoto’s thyroiditis may still have thyroid laboratory values that fall within conventional reference ranges while immune-mediated reproductive disruption continues beneath the surface.
How Thyroid Antibodies May Affect Fertility
Thyroid antibodies do not directly “cause” infertility, but they may reflect a broader immune environment that is less supportive of ovulation, implantation, and early pregnancy development.
Research suggests autoimmune thyroid activity may influence fertility through several mechanisms, including:
Increased inflammatory signaling
Altered endometrial receptivity
Disrupted implantation physiology
Impaired immune tolerance during early pregnancy
Greater physiologic stress on reproductive tissues
These effects may occur even when thyroid hormone levels appear “normal” on standard laboratory testing (11).
In some women, Hashimoto’s thyroiditis may contribute to:
Difficulty getting pregnant
Recurrent miscarriage
Implantation failure
Irregular ovulation
Reduced fertility despite “normal” thyroid labs
Variable IVF outcomes
Importantly, antibody positivity does not necessarily indicate irreversible thyroid damage. Immune activation exists on a spectrum and may fluctuate over time depending on inflammatory burden, stress physiology, nutrient status, gut health, metabolic function, and broader immune regulation.
→ Immune Health & Autoimmune Support
Autoimmune Thyroid Disease, Implantation, and Early Pregnancy Loss
Successful implantation requires precise immune regulation. During early pregnancy, the immune system must remain active enough to protect against infection while simultaneously shifting into a more tolerant state that allows embryonic implantation and placental development to proceed normally.
In Hashimoto’s thyroiditis and other autoimmune thyroid conditions, immune signaling may become more inflammatory and less tolerant. This altered immune environment has been associated with:
Increased risk of implantation failure
Higher rates of recurrent miscarriage
Reduced implantation support
Greater variability in fertility outcomes
Increased risk of early pregnancy loss
These associations may persist even when thyroid hormone replacement normalizes standard thyroid laboratory markers (11).
This helps explain why some women continue experiencing infertility or miscarriage despite being considered “well-controlled” on thyroid medication.
Why Autoimmune Thyroid Dysfunction Is Often Missed in Fertility Care
Routine fertility evaluations frequently focus on TSH and circulating thyroid hormone levels while overlooking thyroid antibodies and immune-mediated thyroid dysfunction.
As a result, many women with Hashimoto’s thyroiditis or autoimmune thyroid activity may be told their thyroid function is “normal” despite ongoing reproductive dysfunction, implantation difficulties, recurrent miscarriage, or unexplained infertility (12).
Because autoimmune thyroid activity may influence fertility independently of hormone levels alone, thyroid antibodies and immune regulation often need to be evaluated within the broader context of reproductive, metabolic, inflammatory, and endocrine health rather than in isolation.
Can You Have Thyroid-Related Infertility With Normal Thyroid Labs?
Many women experiencing infertility, recurrent miscarriage, irregular ovulation, or difficulty getting pregnant are told their thyroid labs are “normal.” However, standard thyroid testing primarily measures hormone concentrations circulating in the bloodstream—not how effectively thyroid hormones are functioning within reproductive tissues (2).
This distinction is important because fertility depends on functional thyroid signaling at the cellular level, not simply on whether thyroid hormone is present in the blood.
In many cases, women may continue experiencing thyroid-related reproductive dysfunction despite thyroid laboratory values falling within conventional reference ranges.
Hormone Levels vs. Thyroid Hormone Function
For thyroid hormones to properly support fertility, several physiologic processes must occur successfully:
Thyroid hormones must be converted into their active form
Hormones must enter ovarian and uterine cells
Receptors must respond appropriately to hormonal signaling
Cells must generate adequate metabolic and mitochondrial activity
Reproductive tissues must maintain normal hormone responsiveness
Disruption at any of these levels may impair ovulation, implantation, endometrial development, or early pregnancy support without producing obvious abnormalities on standard thyroid blood tests (8).
This helps explain why some women continue struggling with infertility despite being told their thyroid function is “normal.”
Why Reproductive Tissues Are Highly Sensitive to Thyroid Dysfunction
The ovaries and uterus are highly sensitive to thyroid hormone activity. Even relatively small reductions in tissue-level thyroid signaling may affect:
Follicle development
Egg maturation
Ovulation timing
Endometrial receptivity
Progesterone production
Implantation support
Menstrual cycle regulation
These tissue-level effects are not directly measured by standard thyroid panels, which focus primarily on circulating hormone levels rather than local hormone conversion, receptor sensitivity, or cellular responsiveness (8).
As a result, thyroid-related infertility may develop long before overt hypothyroidism becomes detectable through routine laboratory screening.
The Limitations of TSH-Centered Thyroid Testing in Fertility Care
Thyroid-stimulating hormone (TSH) is commonly used as the primary thyroid screening marker, but TSH reflects pituitary signaling rather than direct thyroid hormone activity within reproductive tissues.
In fertility contexts, relying on TSH alone may overlook:
Impaired T4-to-T3 conversion
Reduced tissue responsiveness to thyroid hormones
Inflammatory interference with hormone signaling
Autoimmune thyroid activity
Cellular hypothyroid patterns despite “normal” labs
This helps explain why many women with Hashimoto’s thyroiditis, subclinical hypothyroidism, or functional thyroid dysfunction continue experiencing infertility, implantation difficulties, recurrent miscarriage, or irregular ovulation despite laboratory values that appear normal on paper (6).
→ Advanced Functional Lab Testing
Rather than evaluating thyroid markers in isolation, fertility-focused thyroid assessment often requires considering thyroid hormones within the broader context of reproductive physiology, immune regulation, metabolic health, inflammation, and tissue-level hormone responsiveness.
Why Thyroid Medication Alone May Not Fully Restore Fertility
Thyroid hormone replacement can play an important role in supporting fertility, particularly in women with hypothyroidism or Hashimoto’s thyroiditis. However, normalizing thyroid laboratory markers does not automatically restore ovulation, implantation, reproductive hormone signaling, or pregnancy outcomes (13).
This is because fertility depends not only on circulating thyroid hormone levels, but also on how effectively thyroid hormones function within reproductive tissues.
In many women, thyroid medication improves bloodwork while the broader physiologic environment affecting fertility remains dysregulated.
Thyroid Medication Improves Hormone Availability — Not Always Tissue-Level Function
For thyroid hormones to properly support fertility, they must:
Convert into their active form
Enter ovarian and uterine cells
Bind appropriately to hormone receptors
Support mitochondrial energy production
Function within a stable immune and inflammatory environment
Thyroid medication primarily improves hormone availability within the bloodstream, but it does not directly correct many of the underlying physiologic factors that may impair hormone function at the tissue level (10).
As a result, some women may continue experiencing:
Difficulty getting pregnant
Irregular ovulation
Luteal phase dysfunction
Implantation difficulties
Recurrent miscarriage
Persistent fertility challenges despite “normal” thyroid labs
This helps explain why reproductive dysfunction may persist even when thyroid blood markers improve.
How Inflammation and Autoimmune Activity Can Interfere With Fertility
Inflammation—particularly chronic inflammatory signaling associated with Hashimoto’s thyroiditis or autoimmune thyroid disease—may interfere with thyroid hormone signaling in multiple ways.
Inflammatory and immune-mediated processes may:
Reduce conversion of thyroid hormone into its active form
Impair cellular responsiveness to thyroid hormones
Disrupt mitochondrial energy production
Alter reproductive hormone signaling
Shift physiologic resources away from reproduction and toward survival regulation
From a physiologic perspective, these responses are protective during periods of stress, inflammation, or immune activation. However, they may become counterproductive for ovulation, implantation, and pregnancy support when they remain chronically active (13).
Increasing thyroid hormone dosage alone does not necessarily override these broader regulatory patterns when inflammatory and immune dysfunction remain unresolved.
Why Fertility Symptoms May Persist Despite “Normal” Thyroid Labs
Reproductive tissues are highly sensitive to immune signaling, metabolic stress, mitochondrial function, and tissue-level hormone responsiveness. Even relatively subtle dysregulation may affect:
Ovulation quality
Egg maturation
Progesterone production
Implantation support
Endometrial receptivity
Early pregnancy maintenance
This helps explain why many women continue experiencing infertility, recurrent miscarriage, implantation difficulties, or persistent reproductive symptoms despite being considered “well-controlled” on thyroid medication (13).
In these situations, the issue is often not inadequate thyroid treatment alone, but incomplete physiologic regulation across the broader endocrine, immune, metabolic, and inflammatory systems that influence reproductive function.
Restoring fertility often requires evaluating thyroid hormones within the larger context of immune regulation, inflammation, reproductive physiology, metabolic health, nutrient status, and tissue-level hormone responsiveness rather than focusing exclusively on laboratory normalization alone.
Thyroid Dysfunction, IVF, and Assisted Reproductive Outcomes
Thyroid dysfunction may also influence fertility outcomes during in vitro fertilization (IVF) and other assisted reproductive procedures. Ovulation induction, egg retrieval, fertilization, implantation, and early embryo development all depend on coordinated endocrine, metabolic, and immune signaling—systems that are closely influenced by thyroid hormone activity (14).
Many women undergoing fertility treatment ask whether thyroid problems can affect IVF success rates, implantation, or miscarriage risk during assisted reproductive treatment.
Both hypothyroidism and autoimmune thyroid conditions such as Hashimoto’s thyroiditis have been associated with altered ovarian responsiveness, impaired implantation support, recurrent implantation failure, and increased risk of early pregnancy loss in some women undergoing fertility treatment (14).
Even relatively mild thyroid dysfunction may affect:
Follicle development during ovarian stimulation
Egg maturation and quality
Endometrial receptivity
Implantation physiology
Early placental development
Embryo support during early pregnancy
Thyroid hormones help regulate mitochondrial energy production, metabolic activity, and cellular signaling throughout reproductive tissues. When thyroid hormone signaling becomes impaired, reproductive tissues may become less responsive to the physiologic demands of conception and implantation—even when IVF protocols are otherwise optimized (14).
Hashimoto’s Thyroiditis and Thyroid Antibodies in IVF
Thyroid antibodies—particularly thyroid peroxidase (TPO) antibodies—have also been studied in women undergoing IVF and assisted reproductive treatment.
Research suggests autoimmune thyroid activity may be associated with:
Reduced implantation rates
Increased miscarriage risk
Greater variability in IVF outcomes
Altered immune signaling during early pregnancy
Importantly, these effects may occur even when standard thyroid laboratory values appear within reference ranges (14).
This helps explain why some women undergoing IVF continue experiencing implantation difficulties or recurrent pregnancy loss despite apparently “normal” thyroid bloodwork and appropriate fertility treatment protocols.
Because reproductive outcomes depend on endocrine, immune, metabolic, and inflammatory regulation simultaneously, thyroid function in IVF settings often needs to be evaluated within the broader context of whole-body reproductive physiology rather than through TSH levels alone.
A Systems-Based Approach to Thyroid-Related Infertility
Fertility is not controlled by a single hormone, isolated organ, or laboratory value. Ovulation, implantation, embryo development, and early pregnancy support depend on coordinated communication between the thyroid, ovaries, brain, immune system, metabolism, nervous system, and reproductive hormones.
When thyroid dysfunction contributes to infertility, the issue is often more complex than low thyroid hormone production alone. In many women, reproductive dysfunction involves multiple overlapping factors affecting how thyroid hormones are:
Converted into active forms
Transported into reproductive tissues
Interpreted at the cellular level
Integrated with ovarian and reproductive hormone signaling
Influenced by inflammation, stress physiology, and immune regulation
This helps explain why many women continue experiencing infertility, recurrent miscarriage, implantation difficulties, irregular ovulation, or persistent reproductive symptoms despite “normal” thyroid laboratory values or thyroid medication alone (7).
From a physiologic perspective, reproduction requires the body to perceive sufficient metabolic stability, immune balance, nutrient availability, and hormonal coordination to support pregnancy safely. When inflammatory, endocrine, metabolic, or immune dysfunction remain unresolved, reproductive signaling may become deprioritized even when thyroid bloodwork appears relatively stable.
A systems-based approach recognizes that restoring fertility often involves evaluating thyroid hormones within the broader context of:
Immune regulation
Inflammatory signaling
Ovulatory function
Metabolic health
Mitochondrial function
Nutrient status
Nervous system regulation
Reproductive hormone balance
Rather than focusing exclusively on laboratory normalization alone, this broader framework evaluates the physiologic environment in which ovulation, implantation, and pregnancy signaling occur.
Why Thyroid-Related Fertility Problems Often Develop Gradually
Thyroid-related infertility rarely develops from a single abnormal laboratory value in isolation. More commonly, fertility challenges emerge gradually as subtle dysregulation accumulates across multiple interconnected systems influencing reproductive physiology.
When thyroid hormone signaling becomes impaired—whether from hypothyroidism, Hashimoto’s thyroiditis, inflammation, impaired hormone conversion, metabolic dysfunction, or reduced tissue responsiveness—the reproductive system may begin receiving inconsistent or suboptimal signals over time.
This may contribute to:
Irregular ovulation
Reduced egg quality
Luteal phase dysfunction
Impaired implantation
Recurrent miscarriage
Difficulty maintaining pregnancy
Persistent infertility despite “normal” laboratory values
Because these disruptions are often functional and regulatory rather than structural, many women continue menstruating regularly while reproductive signaling progressively becomes less efficient.
This helps explain why thyroid-related infertility is frequently overlooked during routine screening and why many women continue experiencing persistent difficulty getting pregnant despite being told their thyroid function is “normal.
Approaching thyroid-related fertility concerns through a systems-based lens allows endocrine, immune, inflammatory, metabolic, and reproductive factors to be evaluated together rather than treating thyroid function as an isolated variable.
Thyroid-related infertility is often more complex than a single abnormal laboratory value or isolated hormone imbalance. Ovulation, implantation, egg quality, immune tolerance, and early pregnancy support all depend on coordinated endocrine, metabolic, inflammatory, and immune signaling.
Because thyroid dysfunction may affect fertility long before overt hypothyroidism develops, many women continue experiencing infertility, recurrent miscarriage, implantation difficulties, or persistent reproductive symptoms despite “normal” thyroid laboratory values.
Understanding thyroid-related fertility concerns through a systems-based lens helps explain why evaluating thyroid function in isolation may overlook important physiologic factors influencing reproductive outcomes.
→ Thyroid Health & Hormone Balance
You may request a free 15-minute consultation with Dr. Martina Sturm to review your health concerns and outline appropriate next steps within a root-cause, systems-based framework.
Frequently Asked Questions About Thyroid Disorders and Fertility
Can thyroid problems cause infertility?
Yes. Thyroid disorders can interfere with ovulation, implantation, menstrual cycle regulation, progesterone production, and early pregnancy support. Both hypothyroidism and Hashimoto’s thyroiditis have been associated with infertility, irregular ovulation, recurrent miscarriage, and difficulty getting pregnant—even when thyroid laboratory values appear within conventional reference ranges.
Can hypothyroidism make it harder to get pregnant?
Yes. Hypothyroidism may impair ovulation timing, reduce progesterone production, disrupt menstrual cycle regulation, and interfere with implantation. In some women, fertility may be affected even when hypothyroidism is mild or considered subclinical. Many women experiencing difficulty getting pregnant may have underlying thyroid dysfunction contributing to ovulatory or implantation-related problems
Can you have thyroid-related infertility with normal thyroid labs?
Yes. Standard thyroid testing measures hormone levels circulating in the bloodstream, but fertility depends on how effectively thyroid hormones function within reproductive tissues. Some women experience ovulatory dysfunction, implantation difficulties, or infertility despite thyroid laboratory values that fall within standard reference ranges.
Can Hashimoto’s thyroiditis affect fertility?
Yes. Hashimoto’s thyroiditis and thyroid antibodies have been associated with increased inflammatory signaling, implantation difficulties, recurrent miscarriage, and altered reproductive immune regulation. These effects may occur even when thyroid hormone levels appear normal on standard laboratory testing.
Can thyroid problems cause miscarriage?
Thyroid dysfunction and autoimmune thyroid disease have been associated with increased risk of early pregnancy loss in some women. Impaired thyroid signaling may affect implantation, placental development, progesterone support, and immune tolerance during early pregnancy.
Can thyroid problems affect IVF outcomes?
Yes. Thyroid dysfunction and thyroid autoimmunity may influence ovarian responsiveness, implantation support, embryo development, and miscarriage risk during IVF and assisted reproductive treatment. Even mild thyroid dysfunction may affect reproductive outcomes in some women undergoing fertility treatment.
What thyroid levels are best for fertility?
There is no single thyroid value that guarantees fertility. While TSH is commonly used as a screening marker, fertility depends on tissue-level thyroid hormone activity, hormone conversion, immune regulation, metabolic health, and reproductive hormone signaling. Thyroid markers are often most useful when interpreted within the broader context of reproductive physiology and fertility history.
Should thyroid antibodies be tested when trying to conceive?
In many cases, yes—particularly with unexplained infertility, recurrent miscarriage, Hashimoto’s thyroiditis, autoimmune disease, or persistent symptoms despite normal thyroid labs. Thyroid antibody testing may help identify immune-related thyroid dysfunction that could influence implantation and early pregnancy support.
Why am I still struggling with infertility while taking thyroid medication?
Thyroid medication may improve circulating hormone levels without fully correcting inflammation, immune dysfunction, impaired hormone conversion, metabolic stress, or tissue-level thyroid signaling. In some women, reproductive dysfunction may persist despite normal thyroid laboratory values and appropriate medication dosing.
Still Have Questions?
If the topics above reflect ongoing symptoms or unanswered concerns, a brief conversation can help clarify whether a root-cause approach is appropriate.
Resources
Endocrine Reviews – Thyroid Hormone Action in the Ovary and Female Reproductive Physiology
Nature Reviews Endocrinology – Tissue-Level Thyroid Hormone Signaling and Cellular Responsiveness
The Journal of Clinical Endocrinology & Metabolism – Subclinical Hypothyroidism and Female Fertility Outcomes
Fertility and Sterility – Thyroid Dysfunction, Ovulation, and Implantation Physiology
Gynecological Endocrinology – Thyroid Function, Progesterone Regulation, and Luteal Phase Support
Human Reproduction Update – Limitations of Standard Thyroid Testing in Reproductive Medicine
Endocrine Reviews – Neuroendocrine and Metabolic Regulation of Female Reproductive Function
Molecular Endocrinology – Thyroid Hormone Receptors and Tissue-Level Reproductive Signaling
Endocrine Reviews – Hypothalamic–Pituitary–Ovarian Axis Regulation and Ovulatory Function
Human Reproduction – Thyroid Dysfunction and Ovulatory Hormone Signaling
Trends in Endocrinology & Metabolism – Autoimmune Thyroid Disease, Implantation, and Early Pregnancy Loss
The Journal of Clinical Endocrinology & Metabolism – Thyroid Antibodies and Reproductive Outcomes in Hashimoto’s Thyroiditis
Endocrine Reviews – Inflammation, Thyroid Hormone Conversion, and Reproductive Physiology
Fertility and Sterility – Thyroid Dysfunction, IVF Outcomes, Implantation Failure, and Assisted Reproductive Technology