
Endometriosis Causes, Symptoms, and Treatment (Root-Cause Approach)
Underlying Drivers of Endometriosis: Immune Dysfunction, Progesterone Resistance, Inflammation, and Environmental Exposures

Endometriosis is a chronic inflammatory condition in which endometrial-like tissue grows outside the uterus, driven by immune dysfunction, hormone signaling disruption, and persistent inflammation. It affects an estimated 10–15% of reproductive-aged women and can significantly impact daily life, long-term health, and overall well-being (1).
Chronic pelvic pain, painful periods, fatigue, digestive discomfort, and fertility challenges are not isolated symptoms. In endometriosis, they reflect deeper inflammatory, immune, and hormonal signaling disturbances that extend beyond the reproductive system.
From a functional medicine perspective, endometriosis is a hormonally responsive, immune-mediated inflammatory state that develops and persists when regulatory systems remain disrupted—and may improve when those underlying drivers are addressed.
This article explains the causes of endometriosis, why symptoms often persist despite conventional treatment, and how a functional medicine approach evaluates contributing factors beyond symptom suppression.
What Is Endometriosis and How Does It Develop
Endometriosis is a chronic inflammatory condition in which endometrial-like tissue grows outside the uterus, most commonly affecting the ovaries, fallopian tubes, pelvic peritoneum, and surrounding pelvic structures (2).
This abnormal tissue growth drives inflammation, immune activation, and pain that can extend beyond the reproductive system.
Unlike normal uterine tissue, these endometrial-like implants exhibit altered immune signaling, increased inflammatory activity, and abnormal hormone receptor behavior. This allows them to survive outside the uterus, resist normal immune clearance, and respond to hormonal cycles in a way that promotes persistent inflammation.
Over time, repeated hormonal stimulation leads to tissue irritation, oxidative stress, fibrosis, and adhesion formation. These processes contribute to chronic pelvic pain, organ restriction, and progressive symptoms that do not always correlate with lesion size or imaging findings.
Importantly, endometriosis is not simply misplaced uterine tissue. It is a biologically active, immune-mediated inflammatory condition involving aberrant tissue behavior within a dysregulated biological environment, rather than a purely anatomical problem.
How Endometrial-Like Tissue Behaves Outside the Uterus
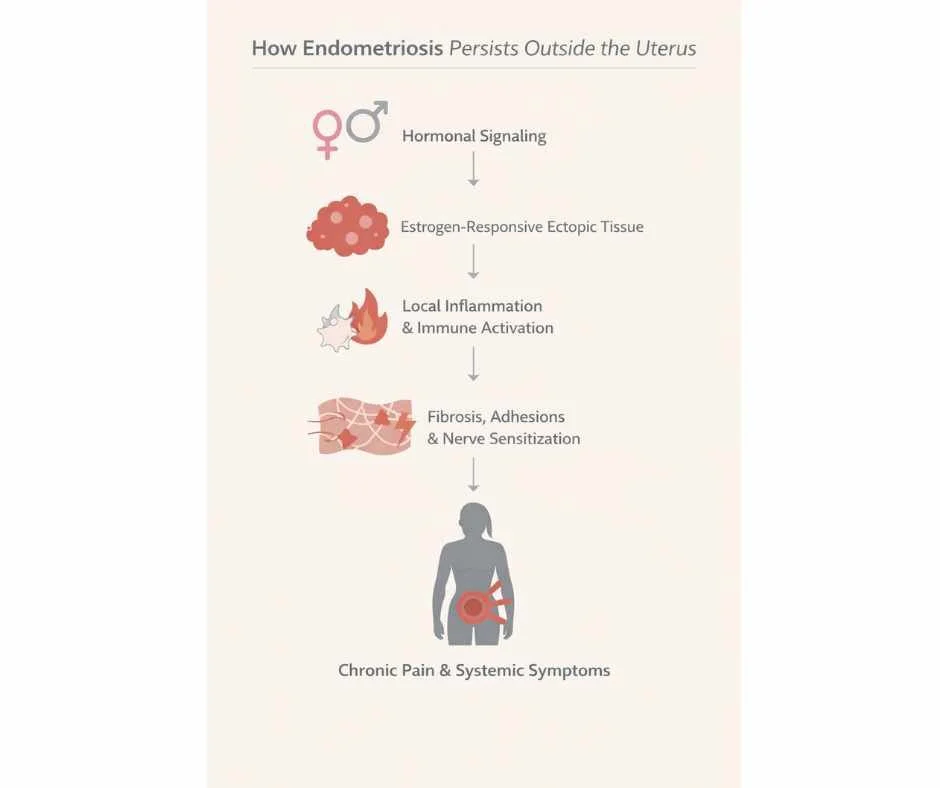
Endometriotic lesions remain hormonally responsive, particularly to estrogen. During the menstrual cycle, these tissues thicken and react to cyclical hormonal signaling in a manner similar to uterine endometrium. However, unlike uterine tissue, ectopic lesions lack a physiologic pathway for breakdown or clearance.
As a result, repeated hormonal stimulation leads to:
Persistent local inflammation
Swelling and oxidative stress
Fibrotic tissue remodeling
Adhesion formation between organs
Over time, this inflammatory cascade contributes to chronic pelvic pain, restricted organ mobility, and progressive symptom burden (3). Inflammatory mediators released by these lesions can also sensitize surrounding nerves, amplifying pain perception even when lesion size is relatively small.
This helps explain why symptom severity does not always correlate with the visible extent of disease.
Why Endometriosis Is More Than a Gynecologic Condition
Although endometriosis is often categorized as a reproductive disorder, current research supports its classification as a systemic, immune-mediated inflammatory condition.
Endometriosis involves:
Altered immune surveillance that fails to clear ectopic tissue
Chronic inflammatory signaling within the pelvic environment
Abnormal hormone receptor responsiveness at the tissue level
Nervous system sensitization that can perpetuate pain beyond the pelvis
These overlapping mechanisms mean that endometriosis affects far more than reproductive anatomy alone. Fatigue, pain amplification, bowel or bladder symptoms, and widespread inflammatory effects reflect the involvement of multiple regulatory systems—not just the uterus or ovaries.
Endometriosis is best understood as a whole-system condition driven by immune, inflammatory, hormonal, and nervous system interactions—not a localized structural disorder.
Understanding endometriosis through this broader biological lens helps explain why symptom-only approaches often fall short and why whole-system evaluation is necessary for meaningful, sustained improvement.
Who Is Most Affected by Endometriosis
Endometriosis affects approximately 1 in 10 women of reproductive age in the United States (4), yet symptoms often begin earlier and may go unrecognized for years.
Many women experience symptoms long before receiving a diagnosis, often navigating pain, fatigue, or cycle-related changes without clear explanation or validation.
Although diagnosis commonly occurs in women in their 30s and 40s, symptoms frequently begin during adolescence or early adulthood. This gap between symptom onset and diagnosis is a defining feature of endometriosis.
A hallmark challenge in endometriosis care is diagnostic delay, with many women waiting an average of 7 to 10 years between initial symptoms and formal diagnosis. During this time, persistent inflammation, lesion progression, and nervous system sensitization may become more established, making symptoms more complex over time.
How Common Is Endometriosis and When Does It Begin
Early symptoms—such as painful periods, pelvic discomfort, fatigue, or gastrointestinal changes—are often normalized or attributed to routine menstrual variation. In other cases, symptoms are treated in isolation without evaluating an underlying inflammatory condition.
These delays are clinically significant. Prolonged untreated inflammation can contribute to:
Lesion persistence
Adhesion formation
Progressive pain sensitization
Broader symptom involvement beyond the pelvis
This helps explain why symptoms may intensify, evolve, or become more difficult to manage over time without appropriate evaluation.
Genetic and Family Risk Factors for Endometriosis
Endometriosis demonstrates a clear familial pattern. Women with a first-degree relative (mother, sister, or daughter) diagnosed with endometriosis have a significantly higher risk of developing the condition themselves (9).
However, genetic susceptibility is not a sole cause. Inherited factors appear to influence:
Immune regulation
Inflammatory signaling pathways
Hormone receptor responsiveness
These variables shape how the body responds to endometrial-like tissue outside the uterus, helping explain why endometriosis can present differently—even among women within the same family.
Endometriosis risk is best understood as the interaction between genetic susceptibility, immune function, inflammatory signaling, and timing of symptom recognition—not a single predictable pathway.
Common Signs and Symptoms of Endometriosis
Common symptoms of endometriosis include pelvic pain, painful periods, fatigue, digestive symptoms, and pain during intercourse, though symptom severity does not always reflect the extent of disease.
Endometriosis presents with a wide range of symptoms, and symptom severity does not reliably correlate with visible disease. Some women with extensive lesions report mild discomfort, while others experience debilitating pain with minimal findings on imaging or surgery.
This variability reflects differences in inflammatory activity, immune response, lesion location, and nervous system sensitization rather than disease burden alone.
Pelvic Pain and Menstrual Symptoms of Endometriosis
Pelvic and menstrual symptoms are the most commonly recognized features of endometriosis and often prompt initial evaluation.
Common pelvic symptoms include:
Painful menstrual cramping that worsens over time
Heavy or prolonged menstrual bleeding
Persistent pelvic pain between cycles
Pain during or after intercourse
Pain with bowel movements or urination during menstruation (5)
Pain patterns may fluctuate across the menstrual cycle and can intensify as inflammatory signaling and tissue irritation accumulate.
Non-Pelvic Symptoms of Endometriosis (Fatigue, Bloating, and More)
Because endometriosis involves inflammatory and immune-mediated processes, symptoms are not always confined to the pelvis.
Non-pelvic symptoms may include:
Chronic fatigue
Low back or hip pain
Abdominal bloating or constipation
Spotting or irregular bleeding between cycles
These symptoms may reflect referred pain, inflammatory spillover, or nervous system involvement, rather than primary disease in those tissues.
Some women experience relatively mild or intermittent symptoms, while others develop progressively worsening pain, fatigue, and functional limitation over time.
Endometriosis symptoms are best understood as the result of interacting inflammatory, hormonal, immune, and nervous system processes—not a single localized condition.
Why Endometriosis Symptoms Can Worsen Over Time
Endometriosis is a chronic inflammatory condition rather than a static gynecologic finding. When the biological drivers that support lesion survival remain unaddressed, inflammatory activity can persist from cycle to cycle—even when symptoms fluctuate.
Over time, repeated inflammatory signaling can alter tissue structure, pain perception, and organ function, contributing to progression that may not be immediately visible on imaging or routine evaluation.
How Endometriosis Causes Inflammation and Adhesion Formation
Persistent inflammation within the pelvic environment promotes fibrosis and adhesion formation, in which connective tissue develops between organs and surrounding structures.
These changes may lead to:
Restricted organ mobility
Altered pelvic biomechanics
Ongoing mechanical tension that amplifies pain patterns (3)
As fibrosis accumulates, tissues may become less responsive to short-term symptom relief strategies, increasing the likelihood of chronic or recurrent pain.
Why Endometriosis Symptoms Persist Despite Treatment
Symptom-focused approaches—such as pain medications or hormonal suppression—may reduce discomfort temporarily but often do not address the immune dysregulation, inflammatory signaling, or lesion persistence that sustain endometriosis activity.
As a result:
Inflammatory processes may continue beneath the surface
Tissue irritation and fibrosis may progress
Nerve sensitization may become more established
This helps explain why symptoms may return, broaden, or intensify over time despite ongoing treatment.
Why Endometriosis Symptoms Can Become More Severe Over Time
Understanding progression reframes endometriosis as a condition that requires upstream evaluation, not simply escalating symptom management.
When underlying drivers are not addressed, symptom patterns often become more complex, more persistent, and less responsive to isolated interventions over time.
This perspective helps explain why many women experience ongoing challenges despite multiple treatments—and why a whole-system approach becomes increasingly important as symptoms evolve.
What Causes Endometriosis (Root Drivers Explained)
Current research suggests that endometriosis develops through the interaction of multiple biological systems, rather than from a single initiating cause. These interacting factors shape how endometrial-like tissue survives outside the uterus, how inflammation is sustained, and why symptoms persist or progress over time.
Rather than acting independently, hormonal signaling, immune regulation, genetic susceptibility, and environmental exposures appear to reinforce one another within the endometriotic environment.
Progesterone Resistance and Estrogen Dominance in Endometriosis
Endometriosis is increasingly understood to involve progesterone resistance, a state in which tissues do not respond appropriately to progesterone’s anti-inflammatory and regulatory effects. When this signaling is impaired, estrogen-responsive tissue activity is less effectively counterbalanced, allowing inflammatory processes and lesion persistence to continue (6).
Importantly, this altered responsiveness occurs at the tissue level, helping explain why circulating hormone levels may appear normal despite ongoing disease activity.
Immune Dysfunction and Chronic Inflammation in Endometriosis
Immune dysregulation plays a central role in endometriosis. Studies examining peritoneal fluid in affected women demonstrate elevated inflammatory cytokines and reduced immune surveillance, limiting the body’s ability to recognize and clear ectopic endometrial-like tissue (8).
This impaired immune response allows lesions to survive in locations where they would normally be eliminated, perpetuating chronic inflammation within the pelvic environment.
Gut Microbiome and Estrogen Metabolism in Endometriosis
Research has identified distinct gut microbiome patterns in women with endometriosis compared to those without the condition. These differences are thought to influence immune communication and estrogen metabolism, potentially contributing to sustained inflammatory signaling and lesion persistence (7).
While the direction of this relationship remains under investigation, these findings highlight the interconnected nature of immune and inflammatory regulation in endometriosis.
Genetic Risk Factors for Endometriosis
Endometriosis demonstrates a clear familial pattern, supporting the presence of genetic susceptibility rather than deterministic inheritance. Identified genetic factors appear to influence inflammatory pathways, immune regulation, and hormone receptor behavior, shaping how the body responds to ectopic tissue rather than directly causing disease (9).
This helps explain why women with similar genetic backgrounds may experience different symptom severity or disease progression.
Environmental Toxins and Endocrine Disruptors in Endometriosis
Environmental exposures also contribute to endometriosis risk. Endocrine-disrupting chemicals, including phthalates, have been detected at higher levels in women with endometriosis (10).
These compounds may interfere with hormonal signaling and immune regulation, further supporting an inflammatory environment that favors lesion survival and disease persistence.
Why Endometriosis Has Multiple Root Causes
Endometriosis is not driven by a single factor but by the interaction of hormonal, immune, genetic, and environmental influences.
Endometriosis is best understood as a systems-based condition in which multiple biological drivers interact to sustain inflammation, hormone signaling disruption, and lesion persistence over time.
This framework explains why symptom-focused treatment alone often fails to produce lasting relief—and why evaluation must extend beyond reproductive anatomy to fully understand the condition.
How Functional Medicine Treats Endometriosis (A Root-Cause Approach)
From a functional medicine perspective, endometriosis is best understood as a hormonally responsive, immune-mediated inflammatory condition that develops and persists within a complex biological environment. Rather than viewing lesions as isolated anatomical abnormalities, this approach examines the regulatory systems that allow endometrial-like tissue to survive, trigger inflammation, and generate pain over time.
This broader lens helps explain why symptom patterns vary widely between women and why disease activity may continue even when conventional treatments appear effective on the surface.
Why Endometriosis Symptoms Persist With Conventional Treatment
Conventional management strategies—including NSAIDs, hormonal suppression, and surgical intervention—may reduce pain or lesion burden temporarily. However, these approaches often focus on downstream effects rather than the upstream drivers that sustain endometriosis activity.
When immune dysregulation, inflammatory signaling, or environmental influences remain unaddressed, lesion persistence and symptom recurrence become more likely. This helps explain why many women experience incomplete relief, recurrent pain, or progressive symptoms despite multiple interventions (11–14).
A Whole-System Approach to Evaluating Endometriosis
Functional evaluation considers how multiple regulatory systems interact in the context of endometriosis, including:
Hormonal signaling at the tissue level
Immune regulation and inflammatory activity
Detoxification capacity and environmental load
Nervous system sensitization and pain amplification
Rather than applying standardized protocols, this framework prioritizes identifying which contributors are most relevant and how they interact to influence symptom expression and disease progression.
Care at Denver Sports and Holistic Medicine is grounded in this systems-based approach, with evaluation focused on understanding the specific drivers influencing endometriosis activity and determining appropriate next steps.
→ Women’s Health & Fertility Support
Supportive Treatment Strategies for Endometriosis (Functional Medicine Approach)
Functional approaches to endometriosis emphasize supporting regulatory systems rather than suppressing symptoms in isolation. The goal is not to override physiology, but to reduce biological stressors that perpetuate inflammation, tissue irritation, and pain signaling over time.
These strategies are used within a broader clinical framework and are individualized based on symptom patterns, tolerance, and overall health context. Importantly, they are not applied as standalone fixes, but as part of coordinated, systems-based care.
Pain Relief and Inflammation Support for Endometriosis
Chronic inflammation plays a central role in endometriosis-related pain and symptom persistence. Certain botanical compounds—such as curcumin, ginger, and boswellia—have demonstrated anti-inflammatory effects comparable to nonsteroidal anti-inflammatory drugs in some studies, without the same degree of gastrointestinal risk (11,12,16).
Within functional care, these agents are used to modulate inflammatory signaling and reduce pain amplification, rather than simply masking discomfort.
Antioxidant and Cellular Support in Endometriosis
Oxidative stress has been implicated in lesion persistence and inflammatory amplification in endometriosis. Nutrients including vitamins A, C, and E, along with compounds such as N-acetylcysteine and green tea polyphenols, support cellular resilience in inflammatory environments (13,15).
This approach focuses on reducing cumulative tissue stress and protecting against ongoing inflammatory damage, rather than directly targeting lesions.
Liver Detoxification and Estrogen Metabolism Support
Hormonal signaling in endometriosis is influenced by how effectively estrogen is metabolized and cleared. These processes rely on adequate nutrient availability and bile flow. B vitamins and lipotropic compounds support these biochemical pathways and are often considered within a functional framework (17,18).
This support is context-dependent, integrated into broader assessment findings, and not applied uniformly across women.
Acupuncture for Endometriosis Pain and Nervous System Regulation
From a Traditional Chinese Medicine perspective, endometriosis-related pain is often understood through patterns involving blood stasis, constrained circulation, inflammation, and nervous system dysregulation.
Acupuncture has been shown to influence pain signaling, inflammatory mediators, and autonomic nervous system balance, making it a valuable supportive modality in endometriosis care (14). By improving local circulation and regulating nervous system activity, acupuncture may help reduce pain intensity, decrease pelvic tension, and support overall symptom regulation over time.
Within an integrative framework, acupuncture supports pain modulation, circulation, and inflammatory balance—mechanisms that, when underlying drivers are addressed, may contribute to significant symptom improvement and, in some cases, remission.
When to Seek Help for Endometriosis and What to Do Next
Living with endometriosis can be physically and emotionally exhausting—especially when symptoms persist despite treatment and answers remain unclear. When care focuses only on symptom control, it can be difficult to understand why progress feels limited or inconsistent.
When underlying drivers of endometriosis are not evaluated, symptom patterns often remain unresolved despite multiple interventions.
A more complete approach to endometriosis treatment involves identifying the factors contributing to inflammation, hormone signaling disruption, immune dysfunction, and pain amplification.
You may request a free 15-minute consultation with Dr. Martina Sturm to review your health concerns and outline appropriate next steps within a root-cause, systems-based framework.
Frequently Asked Questions About Endometriosis
What are the early signs of endometriosis?
Early signs of endometriosis often include painful periods, pelvic pain that worsens over time, pain during intercourse, bloating, fatigue, and bowel discomfort during menstruation. Many women experience symptoms for years before diagnosis, as these signs are frequently mistaken for normal menstrual changes.
Can endometriosis cause infertility?
Endometriosis can affect fertility by disrupting ovulation, altering pelvic anatomy, and increasing inflammation within the reproductive environment. Adhesions, immune dysfunction, and hormone signaling changes may interfere with fertilization and implantation, although many women with endometriosis are still able to conceive depending on severity and overall health.
Why does endometriosis cause severe pain?
Pain in endometriosis is driven by inflammation, nerve sensitization, tissue irritation, and adhesion formation—not just lesion size. Inflammatory mediators can amplify pain signaling, which explains why some women experience severe symptoms even with minimal visible disease.
Can you have endometriosis with normal hormone levels?
Yes. Endometriosis is often a tissue-level hormone signaling condition involving progesterone resistance and altered estrogen responsiveness. Blood tests may appear normal even when symptoms persist, because they do not reflect receptor activity or local tissue behavior.
Does endometriosis get worse over time?
Endometriosis can progress when inflammation, immune dysfunction, and fibrosis continue without intervention. Symptoms may worsen, expand beyond the pelvis, or become more persistent over time, even if imaging findings do not change significantly.
Can endometriosis cause bloating and digestive symptoms?
Yes. Endometriosis commonly causes bloating, constipation, painful bowel movements, and abdominal discomfort, particularly around the menstrual cycle. These symptoms may result from pelvic inflammation, lesion location, or nervous system involvement.
Is endometriosis an autoimmune disease?
Endometriosis is not classified as an autoimmune disease, but it involves immune dysfunction. Altered immune surveillance and increased inflammatory signaling contribute to the persistence of endometrial-like tissue outside the uterus.
What causes endometriosis?
Endometriosis develops through a combination of factors, including progesterone resistance, chronic inflammation, immune dysregulation, genetic susceptibility, gut microbiome influences, and exposure to endocrine-disrupting chemicals.
Why is endometriosis often diagnosed late?
Endometriosis is often diagnosed late because symptoms such as painful periods, fatigue, and bloating are frequently normalized or treated separately. Many women are told symptoms are “normal,” delaying appropriate evaluation for years.
Can endometriosis symptoms improve without surgery?
In some cases, symptoms can improve when inflammation, hormone signaling, immune function, and nervous system regulation are addressed. While non-surgical approaches do not remove lesions, they may reduce symptom severity and improve overall function.
Still Have Questions?
If the topics above reflect ongoing symptoms or unanswered concerns, a brief conversation can help clarify whether a root-cause approach is appropriate.
Resources
StatPearls Publishing – Endometriosis
Office on Women’s Health – Endometriosis
Human Reproduction Update – Endometriosis: inflammatory mechanisms and fertility implications
Yale Medicine – Endometriosis
Mayo Clinic – Endometriosis: Symptoms and Causes
Endocrine Reviews – Progesterone resistance in endometriosis
Reproductive Sciences – Association between endometriosis and gut microbiota: systematic review and meta-analysis
Frontiers in Immunology – Peritoneal immune microenvironment of endometriosis: role of innate and adaptive immunity
Human Reproduction Update – Genome-wide association studies in endometriosis: systematic review
Environmental Health Perspectives – Phthalate exposure and risk of endometriosis: systematic review and meta-analysis
Journal of Alternative and Complementary Medicine – Comparison of ginger, mefenamic acid, and ibuprofen for dysmenorrhea pain
Gynecological Endocrinology – Melatonin and endometriosis-associated pain: clinical evidence
PLOS ONE – Acupuncture for endometriosis: systematic review and meta-analysis
Gynecological Endocrinology – Efficacy of N-acetylcysteine on endometriosis-related pain and ovarian endometriomas
Phytotherapy Research – Curcumin and endometriosis: anti-inflammatory and antiproliferative effects
Gynecological Endocrinology – Antioxidant therapy with N-acetylcysteine, alpha-lipoic acid, and bromelain in endometriosis-associated pelvic pain