

Most Common Nutrient Deficiencies (Even With Normal Labs)
How absorption issues, metabolic demand, inflammation, and medication use contribute to persistent nutrient deficiencies
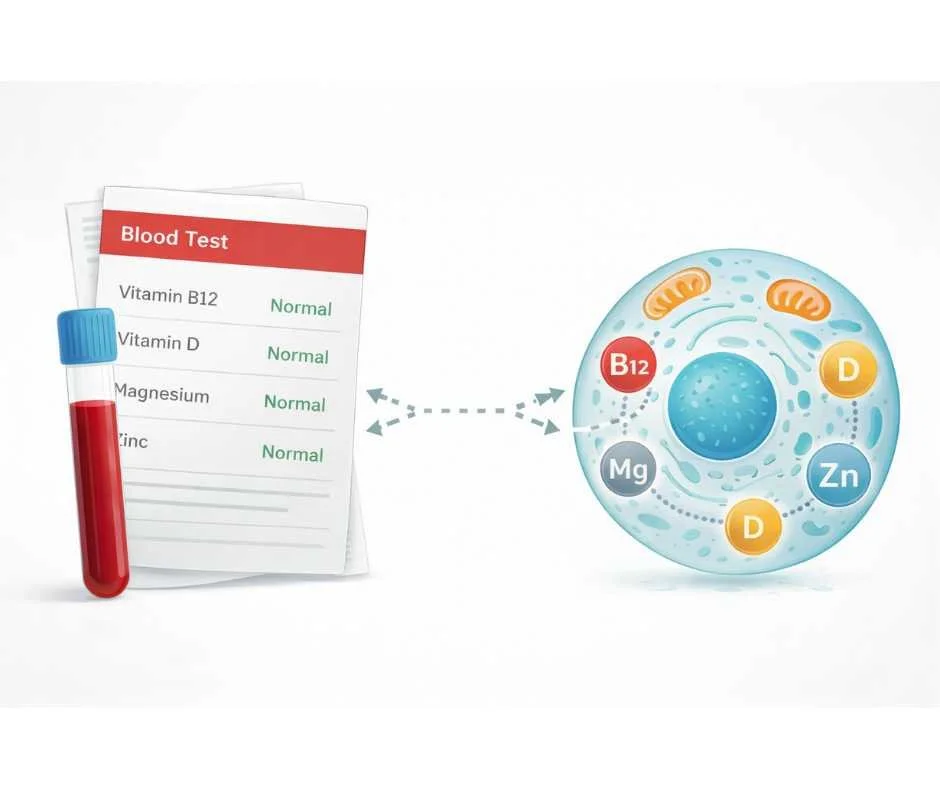
Nutrient deficiencies are among the most common yet frequently overlooked contributors to fatigue, brain fog, immune dysregulation, and metabolic dysfunction—even when routine blood work appears normal (1).
The most common nutrient deficiencies in adults include magnesium, vitamin D, B vitamins (especially B12), iron dysregulation, and zinc insufficiency. These imbalances often develop despite adequate dietary intake and routine medical care (2).
In modern clinical practice, deficiencies rarely reflect poor diet alone. They more often emerge from impaired absorption, increased physiological demand, medication effects, gut dysfunction, chronic inflammation, and environmental stressors.
Nutrient sufficiency is determined by more than intake. Digestive capacity, intestinal integrity, stomach acid production, bile flow, transporter function, metabolic demand, and inflammatory burden all influence whether nutrients reach cells and are effectively utilized. When these systems are disrupted, functional deficiencies can develop even when standard laboratory values fall within reference ranges.
This explains why many individuals are told their labs are “normal” despite ongoing symptoms. Serum measurements reflect circulating nutrients at a single point in time, but they do not reliably assess intracellular availability or increased physiological demand.
Modern conditions further compound this issue. Agricultural soil depletion has reduced micronutrient density in many foods, while chronic stress, toxic exposure, and inflammatory load increase nutrient requirements (3). Certain medications and gastrointestinal disorders can quietly impair absorption or alter metabolism without obvious early symptoms.
For these reasons, nutrient deficiencies are best understood as systems-based disruptions rather than isolated dietary failures. Identifying why they develop—and why they are often missed—requires evaluating intake, absorption, utilization, and metabolic demand together.
“Optimal nutrition is the medicine of tomorrow.”
— Linus Pauling
Why Nutrient Deficiencies Are So Common Today
The rise in nutrient deficiencies is not accidental. It reflects a predictable mismatch between increased physiological demand and reduced nutrient availability, compounded by impaired absorption and metabolic stress (4).
Dietary intake remains relevant—but it is only one component of nutrient sufficiency. In clinical practice, adequacy depends on the interaction between intake, digestive function, absorption, intracellular utilization, metabolic demand, and regulatory resilience. When these variables become misaligned, deficiencies can develop even in individuals who appear to be eating well.
Intake Alone Does Not Prevent Nutrient Deficiency
Recommended dietary allowances were designed to prevent overt deficiency diseases—not to define optimal status for immune regulation, mitochondrial energy production, hormone signaling, or detoxification capacity (5).
These population-based estimates do not account for age-related changes, chronic stress, inflammation, medication use, toxic burden, or individual metabolic variability. As a result, individuals may meet general dietary guidelines while remaining functionally deficient at the tissue level.
Declining Micronutrient Density in Modern Food
Agricultural soil depletion, crop selection for yield, and food processing have reduced the concentration of essential minerals and vitamins in many foods compared to historical baselines (6).
Even diets rich in whole foods may fail to provide sufficient micronutrient density when physiological demand is elevated.
Increased Nutrient Demand From Stress and Inflammation
Chronic stress, immune activation, environmental toxin exposure, and metabolic dysregulation increase the body’s reliance on micronutrients that support antioxidant defense, detoxification pathways, and mitochondrial energy production (7).
When demand rises without proportional replenishment, nutrients are preferentially allocated to short-term survival processes—leaving other systems under-supported.
Absorption Problems Commonly Drive Nutrient Deficiencies
Adequate intake does not guarantee cellular sufficiency. Gastric acid production, bile flow, intestinal integrity, transporter function, and enzymatic activity determine whether nutrients reach target tissues.
Medications, gastrointestinal dysfunction, dysbiosis, and chronic inflammation frequently impair absorption and intracellular utilization (8).
For these reasons, the most common nutrient deficiencies today are best understood as systems-level disruptions—not simple dietary shortcomings.
These patterns help explain why the most common nutrient deficiencies today often persist despite adequate diet and routine testing.
Why Nutrient Deficiencies Are Often Missed on Standard Lab Testing
One of the primary reasons the most common nutrient deficiencies persist is not lack of awareness, but limitation of assessment. Conventional laboratory testing is designed to identify overt disease states rather than early or functional insufficiency (9).
Most standard panels measure circulating serum levels at a single point in time. While these values can identify advanced deficiency, they do not reliably reflect intracellular availability, tissue-level utilization, or increased physiological demand (10).
Serum Levels Do Not Reflect Functional Sufficiency
Serum measurements indicate what is present in the bloodstream—not what is reaching cells, where nutrients are required for mitochondrial energy production, immune regulation, hormone signaling, and detoxification. The body tightly regulates blood concentrations, often maintaining values within reference ranges even when tissues are under-supplied (11).
As a result, functional nutrient depletion can exist long before laboratory values fall outside of “normal” limits.
Increased Demand Is Often Overlooked
Nutrient deficiency does not always reflect inadequate intake. In many cases, physiological demand increases due to chronic stress, inflammation, immune activation, medication use, or environmental exposure. Under these conditions, nutrients are consumed more rapidly or redirected into protective pathways, reducing availability for other metabolic processes (12).
Standard laboratory testing does not account for this elevated demand, leading to false reassurance when values appear acceptable.
Absorption and Utilization Are Rarely Evaluated
Digestive capacity, gut integrity, enzymatic activity, and transporter function all influence whether nutrients are absorbed and effectively utilized. Gastrointestinal dysfunction, hypochlorhydria, dysbiosis, and medication effects can significantly impair assimilation without producing clear abnormalities on routine serum testing (13).
When absorption or intracellular utilization is compromised, increasing intake alone does not resolve deficiency—and standard labs frequently fail to reveal the underlying barrier.
Functional Testing Provides Broader Clinical Context
Functional and cellular micronutrient testing evaluates nutrient status closer to where nutrients are actually used. This approach considers metabolic demand, inflammatory burden, toxic exposure, and cofactor relationships rather than relying solely on serum values (14).
For individuals experiencing persistent symptoms despite “normal” labs, this broader assessment is often necessary to identify clinically meaningful nutrient imbalances.
The Most Common Nutrient Deficiencies in Modern Clinical Practice
Rather than isolated deficiencies, modern clinical patterns more often reflect clusters of insufficiency driven by impaired absorption, increased metabolic demand, inflammatory burden, and regulatory disruption.
The most common nutrient deficiencies observed today include magnesium, vitamin D, B vitamins (particularly B12), iron dysregulation, and zinc insufficiency. These nutrients are repeatedly identified in functional assessment and are especially vulnerable to modern dietary patterns and metabolic stress.
Magnesium (High Demand, Often Underrecognized)
Magnesium plays a central role in ATP production, neuromuscular signaling, glucose regulation, and stress response. Insufficiency is common due to reduced dietary intake, soil depletion, increased losses from chronic stress, and medication use. Serum magnesium is tightly regulated and may not reflect intracellular availability (15).
As a key cofactor, magnesium also influences activation and utilization of other nutrients, including vitamin D.
Vitamin D (Widespread Insufficiency)
Vitamin D insufficiency is consistently observed across populations and is influenced by limited sun exposure, indoor lifestyles, geographic factors, age-related changes in synthesis, and impaired absorption of fat-soluble nutrients (16).
Because vitamin D functions as a hormone precursor involved in immune regulation, neuromuscular signaling, and calcium metabolism, inadequate status often reflects broader regulatory strain rather than simple intake failure.
B Vitamins (Demand, Absorption, and Interdependence)
B vitamins function as interconnected pathways supporting mitochondrial energy production, neurotransmitter synthesis, methylation, and detoxification. Functional insufficiency frequently reflects increased demand from chronic stress or inflammation, impaired absorption due to gastrointestinal dysfunction, or medication effects rather than inadequate intake alone (17).
Vitamin B12 is particularly sensitive to disruptions in stomach acid production and intrinsic factor availability.
Iron Dysregulation (Utilization and Regulation)
Iron status is frequently mischaracterized as a simple deficiency problem. In many cases, iron is present but poorly utilized due to inflammatory signaling, immune activation, gastrointestinal dysfunction, or impaired regulation (18).
Iron concerns are therefore best evaluated within a broader inflammatory and metabolic context rather than addressed through intake alone.
Zinc (Absorption and Immune Demand)
Zinc supports immune signaling, epithelial integrity, and enzymatic activity. Insufficiency may develop in the setting of gastrointestinal dysfunction, chronic inflammation, or increased immune demand. Because zinc absorption occurs primarily in the small intestine, disruptions in gut health can significantly affect status even when dietary intake appears adequate (19).
Why Nutrient Deficiencies Persist Despite Adequate Diet and Normal Labs
Across these nutrients, a clear pattern emerges: deficiency rarely reflects intake alone. Instead, insufficiency develops through the interaction between dietary availability, digestive and absorptive capacity, metabolic demand, inflammatory burden, and cofactor dependency.
This explains why the most common nutrient deficiencies today frequently persist despite adequate dietary intake and routine laboratory testing.
This systems-based dynamic is precisely why conventional testing alone often fails to identify clinically meaningful nutrient imbalance.
How Nutrient Deficiencies Should Be Evaluated
Because the most common nutrient deficiencies are rarely driven by intake alone, evaluation must extend beyond symptoms and basic laboratory panels. Effective assessment considers where nutrient breakdown occurs—intake, absorption, intracellular utilization, or regulatory demand—rather than assuming a single point of failure.
Why Symptoms Alone Cannot Diagnose Nutrient Deficiency
Symptoms of nutrient insufficiency are often non-specific and overlapping. Fatigue, cognitive changes, immune shifts, and metabolic disturbances may reflect inflammation, hormonal dysregulation, mitochondrial stress, or impaired absorption. Without objective assessment, it is difficult to determine which nutrients are involved—or whether imbalance is primary or secondary.
Why Standard Blood Tests Miss Nutrient Deficiencies
Conventional laboratory panels are designed to detect severe deficiency states and overt disease. Most assess circulating serum levels at a single point in time. While useful for identifying advanced deficiency, serum values do not reliably reflect intracellular availability, functional utilization, or increased physiological demand.
Because nutrients are required inside the cell—where they support mitochondrial energy production, enzymatic reactions, immune signaling, and detoxification—the bloodstream serves primarily as a transport compartment. The body tightly regulates serum concentrations, allowing clinically meaningful insufficiency to persist despite “normal” lab results.
Absorption and Metabolic Demand Are Rarely Measured
Digestive capacity, gut integrity, bile flow, enzymatic activity, and transporter function determine whether nutrients reach tissues. Gastrointestinal dysfunction, chronic inflammation, medication use, and metabolic stress can impair intracellular uptake or accelerate depletion without obvious serum abnormalities.
In these cases, increasing intake alone does not resolve deficiency.
Functional and Cellular Testing Provides Deeper Insight
Functional and micronutrient testing evaluates nutrient status closer to where nutrients are utilized. This approach interprets results within the context of metabolic demand, inflammatory burden, toxic exposure, and cofactor relationships rather than relying solely on serum values.
→ Advanced Functional Lab Testing
Why Testing Should Precede Supplementation
Targeted correction is most effective when it follows comprehensive evaluation. Addressing nutrient imbalance without understanding intracellular availability, absorption barriers, and cofactor dependencies can produce incomplete results or unintended imbalance.
Testing before treatment allows correction to be precise, proportional, and aligned with the broader physiological context—supporting durable restoration rather than temporary compensation.
Why Nutrient Deficiencies Persist Despite “Normal” Labs and Supplement Use
Nutrient deficiencies rarely occur in isolation and are seldom explained by diet alone. In modern clinical patterns, insufficiency most often reflects a mismatch between intake, absorption, intracellular utilization, metabolic demand, and cofactor availability—variables that standard evaluation frequently fails to capture.
This explains why the most common nutrient deficiencies often persist despite “normal” laboratory results, well-intentioned supplementation, or adherence to general dietary guidelines. When nutrients fail to reach the cell—or cannot be effectively utilized once there—replacement alone does not correct the underlying imbalance.
A systems-based approach shifts the focus from guessing or blanket supplementation toward identifying where regulation is breaking down. By evaluating nutrient status within the context of metabolic demand, inflammatory burden, digestive function, and cofactor relationships, correction becomes more precise, proportional, and durable.
Effective resolution requires moving beyond symptoms and isolated lab values toward a comprehensive assessment of how the body is functioning as an integrated system.
When Deeper Nutrient Evaluation Is Clinically Warranted
Persistent fatigue, cognitive changes, digestive dysfunction, chronic inflammation, or long-term medication use may indicate that routine laboratory testing is insufficient to fully assess nutrient status.
→ Functional & Integrative Medicine
You may request a free 15-minute consultation with Dr. Martina Sturm to review your health concerns and outline appropriate next steps within a root-cause, systems-based framework.
Frequently Asked Questions About Nutrient Deficiencies
What are the most common nutrient deficiencies in adults?
The most common nutrient deficiencies include magnesium, vitamin D, vitamin B12 and other B vitamins, iron dysregulation, and zinc insufficiency. These deficiencies often develop due to impaired absorption, increased metabolic demand, inflammation, medication use, or chronic stress—not diet alone.
Can you have nutrient deficiencies even if your blood tests are normal?
Yes. Standard blood tests measure circulating serum levels, not intracellular availability. The body tightly regulates blood concentrations, which means nutrient deficiencies can exist at the cellular level despite “normal” lab results.
Why do nutrient deficiencies persist despite taking supplements?
Deficiencies may persist when nutrients are not properly absorbed, transported, or utilized inside cells. Missing cofactors, impaired digestion, inflammation, or increased metabolic demand can prevent supplements from restoring true intracellular sufficiency.
What causes nutrient deficiencies besides poor diet?
Common causes include gut dysfunction, low stomach acid, bile flow issues, chronic inflammation, stress, medication use, toxic exposure, and increased metabolic demand. Many nutrient deficiencies result from impaired absorption or utilization rather than inadequate intake.
How are nutrient deficiencies properly evaluated?
Accurate evaluation considers intake, absorption, intracellular utilization, metabolic demand, and cofactor relationships. Functional or cellular micronutrient testing can provide a more comprehensive assessment than serum testing alone.
When should you consider deeper nutrient testing?
Deeper testing may be warranted if you have persistent fatigue, brain fog, digestive issues, chronic inflammation, long-term medication use, or ongoing symptoms despite normal labs and supplementation.
Still Have Questions?
If the topics above reflect ongoing symptoms or unanswered concerns, a brief conversation can help clarify whether a root-cause approach is appropriate.
Resources
Nutrients – Global prevalence of micronutrient deficiencies and implications for health
American Journal of Clinical Nutrition – Functional indicators of nutrient status beyond dietary intake
Journal of Nutrition – Effects of modern agricultural practices on micronutrient density of foods
Physiological Reviews – Stress, inflammation, and micronutrient demand in human health
National Academies of Sciences, Engineering, and Medicine – Dietary reference intakes: Applications in clinical practice
Clinical Chemistry – Limitations of serum biomarkers for assessing micronutrient status
Journal of Internal Medicine – Inflammation-mediated alterations in micronutrient metabolism
Journal of Trace Elements in Medicine and Biology – Magnesium deficiency: Mechanisms, assessment, and clinical relevance
Nutrients – Functional B-vitamin deficiencies and medication-related depletion
Nutrients – Zinc absorption, immune demand, and gastrointestinal influences