
Hormonal Birth Control Explained: How It Affects Ovulation, Hormone Balance, and Long-Term Regulation
How the Pill, Hormonal IUDs, and Contraceptives Suppress Ovulation and Alter Hormone Signaling
Hormonal birth control is often presented as a simple solution — a way to regulate cycles, ease PMS, prevent pregnancy, or “balance hormones.” But what does birth control actually do to your hormones?
For many women, birth control pills, hormonal IUDs, patches, and injections are prescribed quickly and early — sometimes before a full ovulatory cycle has even been observed (1). What is rarely explained is that hormonal birth control does not restore hormonal balance. It works by suppressing ovulation and overriding the body’s natural hormone signaling.
Oral contraceptives and other hormonal contraceptives replace endogenous hormone rhythms with synthetic estrogen, synthetic progestins, or both. These compounds alter communication between the brain and ovaries, disrupting the hypothalamic-pituitary-ovarian (HPO) axis and reducing natural progesterone production (2).
Despite being marketed as “low dose” or “local,” hormonal IUDs and other contraceptives exert systemic effects. Progestins enter circulation, bind receptors throughout the body, and influence the brain, liver, breasts, immune system, and nervous system. Ovulation is often suppressed or altered, and endogenous progesterone production declines as a result (3).
In clinical practice, we routinely see women who were placed on hormonal birth control for PMS, acne, irregular cycles, or contraception, only to experience worsening symptoms years later — or significant disruption after stopping birth control. Cycles may become irregular, PMS intensifies, mood shifts emerge, energy drops, and fertility can take time to recover.
Symptom improvement during use is often mistaken for hormonal healing. In reality, many symptoms are masked through suppression rather than resolved at the level of physiology.
This article explains what hormonal birth control does and does not do, how it affects ovulation and hormone signaling, why symptoms may improve temporarily, and what can happen after discontinuation — so women can make informed decisions with a clear understanding of the tradeoffs involved.
How Hormonal Birth Control Suppresses Ovulation and Alters Hormone Signaling
Hormonal birth control works by suppressing ovulation and disrupting the body’s normal reproductive signaling — not by supporting or restoring hormonal balance.
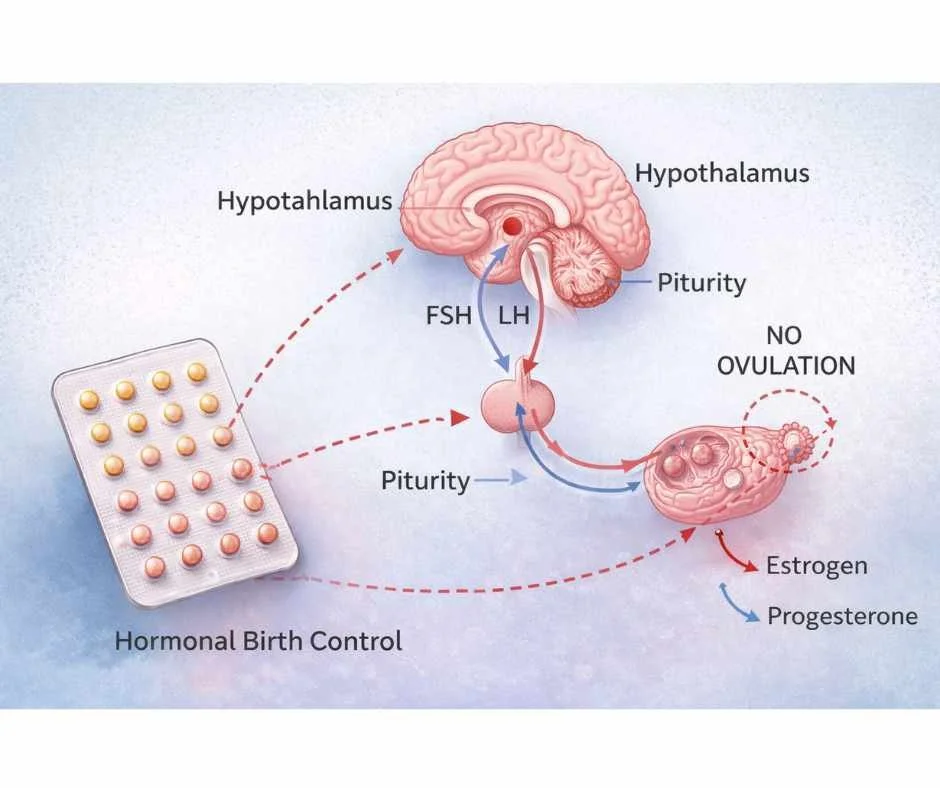
Under normal circumstances, the menstrual cycle is governed by communication between the hypothalamus, pituitary gland, and ovaries — the hypothalamic-pituitary-ovarian (HPO) axis (1). This signaling coordinates ovulation, progesterone production, and the cyclical rise and fall of estrogen that supports mood, metabolism, bone health, and fertility.
Hormonal contraceptives interrupt this process at the top.
Most forms of hormonal birth control — including oral contraceptives, patches, injections, implants, and hormonal IUDs — deliver synthetic estrogen, synthetic progestins, or both. These hormones feed back to the brain and signal that ovulation has already occurred, suppressing follicle-stimulating hormone (FSH) and luteinizing hormone (LH) (2).
When hormonal birth control suppresses this signaling:
Ovulation does not occur consistently or at all
The ovaries reduce endogenous estrogen and progesterone production
Natural progesterone is not produced in meaningful amounts
This suppression is the intended mechanism of action, not a side effect (3).
Because ovulation and progesterone production are central to cycle stability, this mechanism helps explain why birth control is frequently prescribed for PMS, irregular cycles, and period pain.
Synthetic Hormones vs Natural Hormones: Why the Difference Matters
The hormones used in contraceptives are not identical to the hormones the body produces.
Birth control pills and hormonal IUDs use synthetic versions of estrogen and progestin that differ structurally from endogenous estradiol and progesterone. These structural differences affect receptor binding, metabolism, and downstream cellular signaling (4).
Synthetic hormones are designed to resist rapid breakdown and exert sustained receptor activity. Unlike natural hormones, which rise and fall rhythmically, synthetic hormones create a steady pharmacologic exposure.
This distinction matters because hormone receptors are present not only in reproductive tissues, but throughout the brain, liver, gut, breasts, immune system, bones, and cardiovascular system.
As a result, hormonal birth control alters signaling far beyond the uterus or ovaries — an important consideration when evaluating longer-term hormone patterns such as estrogen–progesterone imbalance.
Is the Bleed on Birth Control a Real Period?
Many women are told that birth control “regulates” their period. In reality, the monthly bleed that occurs during placebo weeks or hormone-free intervals is withdrawal bleeding — not a true menstrual period (5).
Withdrawal bleeding reflects a drop in synthetic hormone exposure, not the completion of an ovulatory cycle.
Because ovulation is suppressed, the hormonal events that normally precede menstruation — including progesterone production and coordinated estrogen withdrawal — do not occur.
Hormonal birth control creates a pharmacologic hormone state, not a restored or regulated menstrual cycle.
Understanding this distinction is foundational to any root-cause approach to women’s hormone health.
→ Women’s Health & Fertility Support
What Happens in the Body When Birth Control Suppresses Ovulation
The primary effect of hormonal birth control is ovulation suppression. But ovulation is not only about fertility — it is a signaling event that coordinates progesterone production, brain communication, and metabolic rhythm.
When birth control suppresses ovulation, natural progesterone production does not occur. This shift alters more than the menstrual cycle.
Progesterone supports sleep quality, mood stability, neuroprotection, and inflammatory balance (10,11). Reduced exposure to endogenous progesterone can influence nervous system tone and estrogen balance — particularly in women sensitive to hormonal fluctuations.
Over time, the absence of ovulatory signaling changes how the endocrine system regulates itself.
How Birth Control Replaces Natural Hormone Cycles With Steady Synthetic Exposure
A healthy menstrual cycle depends on fluctuation.
Estrogen rises in the first half of the cycle, ovulation triggers progesterone production, and downstream systems — including cortisol, insulin, and thyroid signaling — adapt dynamically (12).
Birth control replaces this rhythm with continuous synthetic hormone exposure.
Instead of physiologic cycling, the body operates under steady pharmacologic signaling. This dampens feedback loops that regulate receptor sensitivity and hormone responsiveness over time (13).
When stopping birth control, the brain–ovary axis must reestablish cyclical communication. Some women resume ovulation quickly. Others experience irregular cycles, worsened PMS, or delayed progesterone recovery as regulatory systems recalibrate.
How Birth Control Affects Mood, Stress Hormones, and Brain Signaling
The hypothalamus integrates reproductive signaling with stress and metabolic pathways. When ovarian feedback is consistently suppressed, communication within this network shifts (14).
Because this regulation occurs centrally, birth control can influence:
Mood stability
Anxiety patterns
Appetite regulation
Stress tolerance
Energy rhythms
This helps explain why hormonal birth control side effects are often systemic rather than limited to menstrual changes.
How Birth Control Affects the Brain, Bones, and Cardiovascular System
Estrogen and progesterone receptors are distributed throughout the brain, bones, breasts, immune cells, and cardiovascular system (15).
When endogenous hormone production is reduced and replaced with synthetic signaling, tissues adapt to that altered hormonal environment.
Natural cyclic exposure is replaced with steady receptor activation. Over time, this may influence how tissues respond when hormonal birth control is discontinued and physiologic cycling attempts to resume.
Individual responses vary — but the shift from rhythmic endocrine signaling to continuous pharmacologic exposure affects more than reproduction alone.
Why Birth Control Does Not Fix Underlying Hormone Imbalance
Suppressing ovulation does not correct underlying drivers of hormonal dysregulation. It temporarily overrides them.
If stress physiology, metabolic strain, impaired estrogen clearance, or ovulatory dysfunction were present before starting birth control, those drivers remain beneath suppression.
When hormonal birth control is stopped, these underlying factors reemerge. In some cases, symptoms appear intensified because regulatory systems have had limited opportunity to function independently.
Understanding this distinction clarifies why birth control often changes symptoms rather than resolving their root cause — and why restoring hormone balance after discontinuation may require a systems-based approach.
Why Birth Control Symptoms Improve — Then Return After Stopping
One of the most confusing aspects of hormonal birth control is that many women feel better at first.
PMS may lessen. Period pain can decrease. Cycles appear more predictable. Acne improves. Migraines may ease. These changes are often interpreted as evidence that hormones have been “balanced.”
In reality, symptom relief during birth control use reflects suppression — not restoration.
Why Symptoms Improve While on Birth Control
Hormonal birth control reduces hormonal fluctuation.
By suppressing ovulation and flattening the natural rise and fall of estrogen and progesterone, birth control decreases hormonal variability (16). For women whose symptoms are triggered by sensitivity to cyclical hormone shifts, this flattening can temporarily reduce symptom intensity.
The endocrine system becomes quieter — but not necessarily healthier.
How Ovulation Suppression Reduces PMS, Acne, and Migraines
Many common symptoms — including PMS, mood changes, acne, and menstrual migraines — are influenced by the hormonal shifts that occur after ovulation.
When birth control suppresses ovulation, the luteal-phase rise and fall of progesterone does not occur (17). The hormonal signal that normally precedes menstruation is muted.
As a result, symptoms may improve because the triggering fluctuation has been removed.
This explains why symptom relief during birth control use is often:
Incomplete
Inconsistent
Dependent on continued suppression
Why Symptoms Return After Stopping Birth Control
Temporary improvement does not mean underlying drivers have resolved.
Stress physiology, metabolic strain, impaired estrogen clearance, gut disruption, and ovulatory dysfunction may remain present beneath suppression. While birth control is in place, these imbalances are often less noticeable. When stopping birth control, the endocrine system must regulate itself again.
If foundational systems have not been addressed, symptoms frequently return — and in some cases intensify.
This pattern is especially common in women who began hormonal birth control during adolescence or early adulthood, before ovulatory cycles were fully established. When suppression is removed, the body may have limited experience maintaining hormonal rhythm independently.
Why Suppression Does Not Equal Hormone Healing
Relief during hormonal birth control use reflects reduced signaling — not restored regulation.
Understanding this distinction helps explain why birth control can feel beneficial in the short term while creating challenges later, particularly during the transition off.
For many women, the period after stopping birth control reveals the underlying patterns that were temporarily masked.
What Birth Control Does Not Fix: PMS, Acne, Irregular Cycles, and Hormone Imbalance
Hormonal birth control suppresses symptoms — it does not restore physiologic regulation.
Many women are prescribed birth control for PMS, acne, irregular periods, migraines, or mood changes. While symptoms may improve during use, the underlying drivers that created those symptoms often remain active beneath suppression.
Understanding what birth control does not fix helps explain why symptoms frequently return after stopping.
Birth Control Does Not Restore Ovulation
Ovulation is the event that coordinates progesterone production, estrogen balance, and downstream signaling to the brain and body (18).
When birth control suppresses ovulation, the endocrine system is paused rather than repaired. Natural progesterone production does not resume until ovulation resumes. If ovulatory dysfunction was present before starting birth control, it remains uncorrected beneath suppression.
Birth Control Does Not Fix Estrogen Detoxification
Hormone balance depends not only on production, but on clearance.
If estrogen is poorly metabolized or recirculated through the gut, suppressing ovulation does not improve detoxification capacity. In some cases, synthetic hormones increase demand on liver and gut pathways involved in hormone processing (19).
For women with impaired estrogen clearance, symptoms may return once hormonal suppression is removed.
Birth Control Does Not Correct Stress Hormone Imbalance
Chronic stress alters hypothalamic signaling, cortisol rhythm, and ovulatory consistency.
Birth control does not improve stress resilience or nervous system flexibility. It bypasses reproductive signaling while leaving stress physiology unchanged.
If cortisol dysregulation or nervous system strain contributed to cycle disruption, those drivers persist during and after suppression.
Birth Control Does Not Address Insulin Resistance or Metabolic Dysfunction
Metabolic factors such as insulin resistance and blood sugar instability directly influence ovarian signaling and hormone receptor sensitivity.
Birth control does not correct these metabolic drivers. If underlying insulin resistance is present, ovulatory irregularity may return after stopping birth control.
Birth Control Does Not Rebuild Natural Hormone Rhythm
The menstrual cycle is designed to be dynamic.
Cyclical fluctuations in estrogen and progesterone support mood regulation, cognition, immune balance, and metabolic flexibility. Flattening this rhythm may reduce symptoms short term, but it does not retrain the body to regulate hormones independently.
When stopping birth control, the endocrine system must reestablish this rhythm without having practiced it during suppression.
Why Symptoms Often Return After Stopping Birth Control
For these reasons, symptoms frequently return — and sometimes intensify — after discontinuation.
The underlying physiology has not been corrected. In some cases, regulatory systems have had limited opportunity to function autonomously for years.
Understanding what birth control does not fix clarifies why symptom suppression is not the same as hormonal restoration — and why a root-cause, systems-based approach is often required after stopping.
Do Hormonal IUDs Stay Local? Understanding Systemic Effects
Hormonal IUDs are often described as a “localized” form of birth control that works only within the uterus. This framing is incomplete.
Hormonal IUDs release synthetic progestins that enter systemic circulation. While the device is placed in the uterus, the hormone itself does not remain confined there. Progestins are absorbed into the bloodstream and bind to receptors throughout the body — including the brain, breasts, liver, immune system, and nervous system (20).
Because hormone receptors are distributed widely, the effects of a hormonal IUD are not limited to the pelvis.
Do Hormonal IUDs Affect the Whole Body?
Yes.
Progestins used in hormonal IUDs are biologically active compounds designed to alter hormone signaling. Once absorbed into circulation, they influence the hypothalamic-pituitary-ovarian (HPO) axis and broader endocrine feedback loops (21).
Even at low doses, hormones exert physiologic effects. Continuous daily exposure can alter receptor sensitivity and feedback regulation over time — even when measured blood levels appear “low.”
The delivery method is localized. The hormonal signaling is not.
Do Hormonal IUDs Suppress Ovulation?
Many women are told that hormonal IUDs preserve ovulation. In practice, ovulation may be inconsistent, partially suppressed, or functionally altered depending on the individual, duration of use, and baseline physiology (22).
Because progesterone is produced only after ovulation, any disruption in ovulatory signaling directly affects natural progesterone availability.
This helps explain why some women using hormonal IUDs report:
Anxiety
Sleep disturbance
Mood changes
Worsening PMS
Breast tenderness
These symptoms are not random — they reflect altered neuroendocrine signaling.
Hormonal IUD Side Effects Are Often Systemic
Mood changes, decreased libido, headaches, fatigue, and breast tenderness are commonly reported with hormonal IUD use.
These symptoms align with known effects of systemic progestin exposure. When hormone receptors in the brain and other tissues are influenced, whole-body symptoms are expected.
When symptoms appear outside the reproductive system, they are not paradoxical — they are physiologic.
What Happens After Hormonal IUD Removal?
After hormonal IUD removal, experiences vary.
Some women resume ovulatory cycles quickly. Others experience delayed cycle regularity, rebound PMS, acne, mood shifts, or temporary hormonal instability (23).
This variability depends on:
How long ovulation was altered
Baseline hormone resilience
Stress physiology
Metabolic health
Estrogen clearance capacity
Removal stops synthetic hormone exposure — but the endocrine system must reestablish natural rhythm.
Hormonal IUDs may differ in delivery method, but they do not bypass the endocrine system. Understanding this distinction allows women to make informed decisions and contextualize symptoms that are often minimized.
How Birth Control Affects Gut Health, Mood, and Nutrient Levels
Hormonal birth control does not act in isolation. By suppressing ovulation and altering estrogen and progesterone signaling, birth control influences multiple downstream systems — including nutrient metabolism, gut function, detoxification capacity, and mood regulation.
These effects are secondary to altered endocrine signaling, but they help explain why some women experience fatigue, anxiety, bloating, or worsening PMS during or after use.
Can Birth Control Deplete Nutrients?
Hormone metabolism and clearance are nutrient-dependent processes.
Because hormonal birth control introduces continuous synthetic hormone exposure, the body must repeatedly metabolize and detoxify these compounds. This increases demand for key micronutrients, including B vitamins, magnesium, zinc, selenium, and vitamin C — all required for hormone clearance, neurotransmitter production, and stress resilience (24).
Over time, nutrient depletion may impair estrogen metabolism, worsen fatigue, increase anxiety, and reduce the body’s ability to adapt after stopping birth control.
For some women, symptoms become more noticeable after discontinuation because nutrient reserves were gradually depleted during suppression.
Does Birth Control Affect Gut Health and Estrogen Clearance?
Because estrogen metabolism depends partly on gut microbial activity, changes in hormone signaling can influence gut dynamics.
Hormonal contraceptives have been shown to alter gut microbial composition, affecting bacteria involved in estrogen metabolism and clearance (25). Disruption of the estrobolome — the collection of microbes that regulate estrogen deconjugation — may increase estrogen recirculation through beta-glucuronidase activity (26).
This can contribute to persistent estrogenic signaling even when ovarian estrogen production is suppressed.
Clinically, this may present as bloating, constipation, worsening PMS, or cycle irregularity during or after birth control use — particularly in women with preexisting gut vulnerability.
Can Birth Control Affect Mood and Anxiety?
Hormones, gut signaling, and neurotransmitter pathways are tightly interconnected.
Altered estrogen and progesterone signaling can influence serotonin, GABA, and dopamine pathways, while changes in gut integrity may further affect neurotransmitter balance (27,37).
Reduced endogenous progesterone exposure also affects GABAergic tone in the brain, which may contribute to anxiety, sleep disruption, or emotional flattening in susceptible individuals.
These mechanisms help explain why mood symptoms associated with birth control are often systemic rather than purely situational.
Does Birth Control Increase Detoxification Demand?
Synthetic hormones must be metabolized and cleared by the liver and gut.
Chronic exposure increases detoxification demand — particularly in individuals with existing metabolic stress, impaired clearance capacity, or environmental toxin burden (28).
If clearance pathways are overwhelmed, estrogenic metabolites and synthetic hormones may accumulate. This can prolong symptoms during use and contribute to delayed recovery after stopping birth control.
Why These Effects Matter After Stopping Birth Control
These system-level effects do not mean birth control affects every woman the same way. However, they help explain why some women experience more pronounced symptoms during the transition off.
When nutrient depletion, gut disruption, or impaired clearance are present beneath hormonal suppression, symptoms may become more apparent once ovulatory signaling resumes.
Understanding these secondary effects keeps the focus where it belongs: altered endocrine signaling — and how the body adapts during and after suppression.
How to Restore Hormone Balance After Stopping Birth Control
Stopping birth control is not simply about removing synthetic hormones. It is about restoring the body’s ability to regulate ovulation, progesterone production, and hormone rhythm independently.
Post–birth control symptoms are not random. They reflect how well core regulatory systems are functioning after a period of hormonal suppression.
Recovery is less about “detoxing birth control” and more about rebuilding physiologic signaling.
How to Restore Ovulation After Stopping Birth Control
Ovulation must resume for progesterone production, estrogen balance, and cycle stability to return (29).
Restoring ovulation depends on:
Adequate energy availability
Stable blood sugar regulation
Healthy stress signaling
Intact brain–ovary communication
If stress physiology, metabolic dysfunction, or chronic under-fueling are present, ovulatory recovery may be delayed.
How to Balance Estrogen After Stopping Birth Control
Estrogen balance depends not only on production, but on clearance.
After stopping birth control, some women experience persistent PMS, migraines, breast tenderness, or heavy bleeding. In many cases, impaired estrogen metabolism or recirculation amplifies symptoms (30).
Supporting liver detoxification pathways, gut integrity, and estrogen metabolite balance is often essential for smoother hormonal recovery.
How to Rebuild Gut Health and Nutrient Levels After Birth Control
Hormonal suppression can increase nutrient demand and influence gut microbial dynamics.
If nutrient depletion or gut disruption occurred during birth control use, these systems may require intentional repletion and support before hormone signaling normalizes (31).
Magnesium status, B vitamins, zinc, and overall micronutrient sufficiency play meaningful roles in hormone metabolism and nervous system resilience.
How Long Does It Take for Hormones to Regulate After Stopping Birth Control?
There is no universal timeline for hormone recovery after stopping birth control.
Some women resume ovulatory cycles within a few months. Others require more time — particularly if birth control was started during adolescence, used long-term, or layered on top of chronic stress, metabolic strain, or environmental exposures (32).
The duration of suppression and baseline physiologic resilience both influence recovery.
How to Treat Post–Birth Control Hormone Imbalance Naturally
After stopping birth control, hormone imbalance is not random. It reflects disrupted ovulation, altered stress signaling, impaired estrogen metabolism, nutrient depletion, or metabolic dysfunction that became visible once hormonal suppression was removed.
Treating post–birth control hormone imbalance requires restoring physiologic regulation — not re-suppressing symptoms.
A root-cause approach focuses on:
Restoring ovulation and natural progesterone production
Stabilizing blood sugar and insulin signaling
Supporting healthy cortisol rhythm and stress resilience
Improving estrogen metabolism and detoxification pathways
Repleting key micronutrients involved in hormone synthesis
Supporting gut integrity and microbial balance
This approach addresses why symptoms developed in the first place, rather than masking them with another form of suppression.
For some women, hormone balance begins to improve within a few cycles. For others, especially after long-term birth control use, recovery requires more intentional support.
Restoring rhythm — not overriding it — is the goal.
What Happens After Stopping Birth Control — and What to Do Next
Hormonal birth control is often presented as routine, reversible, and benign. For many women, the physiologic reality is more nuanced.
Understanding how birth control suppresses ovulation, alters hormone signaling, affects gut health and nutrient status, and influences nervous system regulation provides important context — especially for women experiencing birth control side effects or symptoms after stopping birth control.
Symptom suppression is not the same as hormonal restoration.
This conversation is not about fear or judgment. It is about informed choice.
Some women use hormonal birth control and feel well. Others notice mood changes, cycle disruption, or difficulty regulating hormones after discontinuation. Both experiences are valid — but informed decisions require an accurate understanding of physiology, tradeoffs, and recovery.
If you are experiencing persistent PMS, irregular cycles, anxiety, fatigue, or post–birth control hormone imbalance, individualized evaluation may help clarify what your body needs next.
You may request a complimentary 15-minute consultation with Dr. Martina Sturm to discuss appropriate next steps and determine whether a root-cause, individualized approach is right for you.
Frequently Asked Questions About Hormonal Birth Control
Does hormonal birth control balance your hormones?
No. Hormonal birth control suppresses ovulation and replaces your body’s natural hormone rhythm with synthetic hormones. While this can reduce symptoms like PMS or acne temporarily, it does not restore natural hormone regulation.
Does birth control stop ovulation completely?
Most forms of hormonal birth control are designed to suppress ovulation. Depending on the method and individual response, ovulation may be fully suppressed or inconsistently disrupted. Without ovulation, natural progesterone production does not occur.
Is the bleed on birth control a real period?
No. The monthly bleed that occurs during placebo or hormone-free intervals is withdrawal bleeding. It reflects a drop in synthetic hormone exposure, not the completion of a natural ovulatory cycle.
Do hormonal IUDs stay local, or do they affect the whole body?
Hormonal IUDs release synthetic progestins that can enter systemic circulation. Although the device is placed in the uterus, the hormone can affect receptors throughout the body, including the brain, liver, and nervous system.
Can birth control cause mood changes or anxiety?
Some women report mood changes, anxiety, or emotional flattening while using hormonal birth control. These effects may be related to altered estrogen and progesterone signaling, as well as changes in neurotransmitter pathways.
Why do symptoms return after stopping birth control?
Birth control suppresses symptoms by flattening hormonal fluctuations. When stopping birth control, ovulation and natural hormone rhythms must resume. If underlying stress, metabolic imbalance, or impaired hormone clearance are present, symptoms may return or temporarily intensify.
How long does it take for hormones to regulate after stopping birth control?
Recovery timelines vary. Some women resume ovulatory cycles within a few months. Others may take longer, especially after long-term use or if underlying hormonal, metabolic, or stress-related imbalances are present.
Can birth control affect gut health and nutrient levels?
Hormonal birth control increases demand for certain nutrients involved in hormone metabolism and may influence gut microbial balance. In some individuals, this can affect estrogen metabolism and overall hormonal resilience.
Still Have Questions?
If the topics above reflect ongoing symptoms or unanswered concerns, a brief conversation can help clarify whether a root-cause approach is appropriate.
Resources
Office on Women’s Health (U.S. Department of Health & Human Services) – Birth Control Methods: Overview and Clinical Use
National Library of Medicine – Mechanisms of action of hormonal contraceptives
National Library of Medicine – Systemic absorption and endocrine effects of hormonal intrauterine devices
Endocrine Reviews – Structural and functional differences between synthetic and endogenous steroid hormones
National Library of Medicine – Withdrawal bleeding versus natural menstruation during oral contraceptive use
Journal of Clinical Endocrinology & Metabolism – Suppression of ovulation and luteal progesterone production by hormonal contraception
Neuroendocrinology – Progesterone’s role in central nervous system regulation and stress modulation
Physiological Reviews – Hormonal feedback loops within the hypothalamic-pituitary-ovarian axis
Frontiers in Endocrinology – Hormonal contraceptives and disruption of endocrine rhythm and feedback sensitivity
Endocrinology – Central regulation of reproductive and metabolic signaling by the hypothalamus
Journal of Women’s Health – Systemic distribution of estrogen and progesterone receptors
Human Reproduction Update – Temporary symptom improvement during hormonal suppression
Psychoneuroendocrinology – Hormonal variability, mood regulation, and menstrual cycle sensitivity
Headache: The Journal of Head and Face Pain – Migraine modulation through ovarian hormone suppression
Fertility and Sterility – Post-contraceptive ovulatory recovery and cycle irregularity
Journal of Steroid Biochemistry & Molecular Biology – Estrogen metabolism and hepatic clearance pathways
Toxicology and Applied Pharmacology – Synthetic hormone burden on liver detoxification systems
Stress – Chronic stress effects on hypothalamic signaling and ovulatory consistency
Metabolism: Clinical and Experimental – Insulin resistance and ovarian hormone signaling
Contraception – Systemic effects of levonorgestrel-releasing intrauterine devices
Journal of Clinical Endocrinology & Metabolism – Progestin feedback effects on ovulation and progesterone
Human Reproduction – Ovulatory patterns in hormonal IUD users
Archives of Women’s Mental Health – Mood and neuroendocrine effects following hormonal IUD removal
Nutrients – Micronutrient depletion associated with long-term hormonal contraceptive use
Gut Microbes – Hormonal contraceptives and alterations in gut microbiome composition
Journal of Gastroenterology and Hepatology – Estrobolome activity and estrogen recirculation
Frontiers in Neuroendocrinology – Progesterone, GABA signaling, and mood regulation
Environmental Health Perspectives – Hormone clearance capacity and cumulative toxic burden
Reproductive Biology and Endocrinology – Restoration of ovulation after hormonal suppression
Obstetrics & Gynecology – Estrogen dominance symptoms following contraceptive discontinuation
Clinical Nutrition – Gut integrity, nutrient status, and hormonal regulation
Best Practice & Research: Clinical Obstetrics & Gynaecology – Long-term endocrine effects of hormonal contraceptive use